inside MSF Ebola treatment centers in Congo amid outbreak
Weeks after Ebola surfaced in both the Democratic Republic of Congo (DRC) and Uganda, Médecins Sans Frontières (MSF) is escalating its efforts to contain the spread. Today, our teams take you inside the treatment centers in Goma and Bunia, Ituri — the outbreak’s ground zero — where staff are battling the seventeenth recorded outbreak of this deadly virus.
Growing outbreak toll demands urgent action
With expanded testing rolled out late last month, the DRC Ministry of Health updated its figures. As of June 4, 2026, the national institute’s records show:
- 381 confirmed cases nationwide;
- 64 confirmed deaths;
- 233 suspected patients currently isolated.
Across the border in Uganda, authorities are monitoring 19 reported cases and one death as of June 5.
MSF expands and reopens Ebola treatment centers
To halt the spread of Bundibugyo virus and break transmission chains, MSF is adapting its response in the hardest-hit zones.
In Bunia: scaling up to meet demand
Bunia’s center is under pressure. By June 5, it was caring for 37 suspected and 7 confirmed patients. To reduce risks of further spread, the facility is expanding quickly. “We are clearing an adjacent plot and will double capacity to 70 beds within days,” says Anthony Kergosien, MSF emergency coordinator in Bunia. If necessary, the center can scale further to 100 beds.
In Goma: reopening a historic facility
In Goma, MSF has reopened a dedicated treatment center to isolate suspected cases and treat confirmed patients. The first admissions began on May 28.
“This center was used in past outbreaks. Our teams start by talking with patients, reassuring them about what to expect, explaining care routines, average length of stay, and the tests they’ll undergo,” explains Tathy Modjaka Nzoko, MSF medical activity manager in Goma.
Protecting staff and winning community trust: the dual challenge
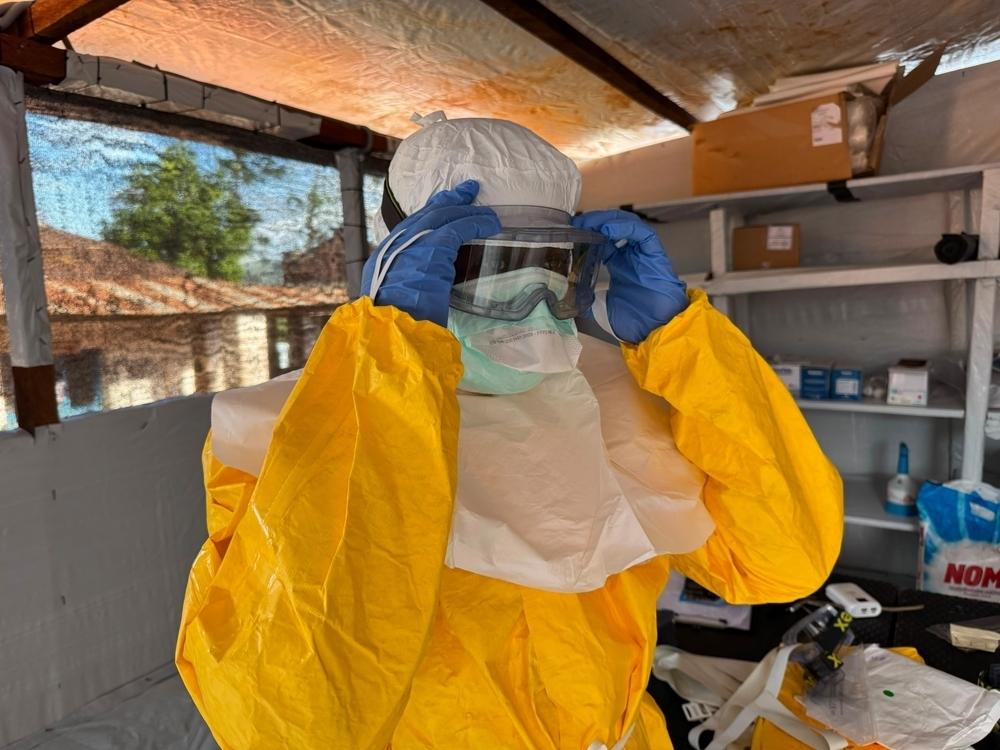
Keeping health workers safe
Medical staff wear full personal protective equipment to guard against Bundibugyo virus. The infectious dose is extremely low. “A few viral particles in the wrong place — eyes or mouth — can trigger illness,” warns Armand Sprecher, MSF emergency physician and epidemiologist.
The gear’s main job is to keep the virus off skin and mucous membranes. “It must be fluid-resistant because the virus travels in bodily fluids. This is critical now because we lack the vaccines and treatments we usually rely on,” he adds.
Winning local support
Convincing sick people to isolate early requires clear communication and trust-building. “Trust between MSF and local communities is vital. Families naturally want to care for loved ones at home, yet we need them to come straight to treatment centers. When people see our staff in protective suits, they may feel uneasy. We explain that many of these suited workers are locals they already know,” Sprecher notes.
Training the next responders
MSF prioritizes knowledge transfer to mount a robust response. Teams receive specialized training at a Belgian center before deployment. “Every Ebola outbreak reinforces the need for knowledge sharing. MSF has staff with deep epidemic-response experience. We send these experts to the field or use them to train others on the ground,” Sprecher explains.
Understanding Bundibugyo virus: why this outbreak is different
Unlike earlier waves in DRC, this outbreak stems from the Bundibugyo Ebola virus (part of the orthoebolavirus family, which includes Zaire and Sudan strains).
While the case fatality rate for Bundibugyo (25–40 %) is lower than for classic Ebola, responders face a major hurdle: no approved vaccine or treatment exists for this strain.
MSF’s ongoing humanitarian push across Congo
Hundreds of MSF staff remain active in Ituri and North Kivu, while new care capacity is being set up in South Kivu. Every week, several tons of medical and logistical supplies arrive in DRC from international hubs to support the intervention.